Tommy Williams, BSN, RN, CCHP
Emily Scordellis, PsyD, CCHP
Correctional health sits at the intersection of health care, mental health services, and custody – three demanding disciplines that must function together even when their priorities do not always align. Among the many challenges this creates, few are more persistent – or more disruptive – than the tension between health care and mental health teams. If unaddressed, that tension can strain relationships, weaken patient care, and worsen the very conditions those involved are trying to treat.
The Problem
Tension often arises from contrasting philosophies, competing priorities, and daily operational differences. Medical teams tend to focus on physical stability, diagnostic results, and infection control, while mental health professionals concentrate on behavioral management, crisis intervention, and long-term psychological wellness.
Both areas of focus are equally important and valid, but their differing approaches can lead to misaligned treatment goals, including disagreements over medication adherence, isolation precautions, the interpretation of somatic complaints, and risk assessments related to self-harm or behavioral escalation. When coordination lapses, critical details can be missed and care can become fragmented, shifting from unified planning to parallel decision-making.
Limited resources and constant time pressure only amplify the divide. Health staff sometimes view mental health interventions as secondary to physical health needs. Conversely, mental health clinicians may see their medical colleagues as dismissive or lacking empathy. Over time, those perceptions can harden, breeding mistrust and professional resentment and ultimately fracturing what should be a unified patient-care team.
ADVERSE EFFECTS ON PATIENT CARE
When tension between teams goes unaddressed, communication becomes transactional instead of collaborative, and patient outcomes suffer. Poor coordination leads to inconsistent care plans, delayed interventions, and a higher risk of missed or inaccurate diagnoses – both medical and psychiatric.
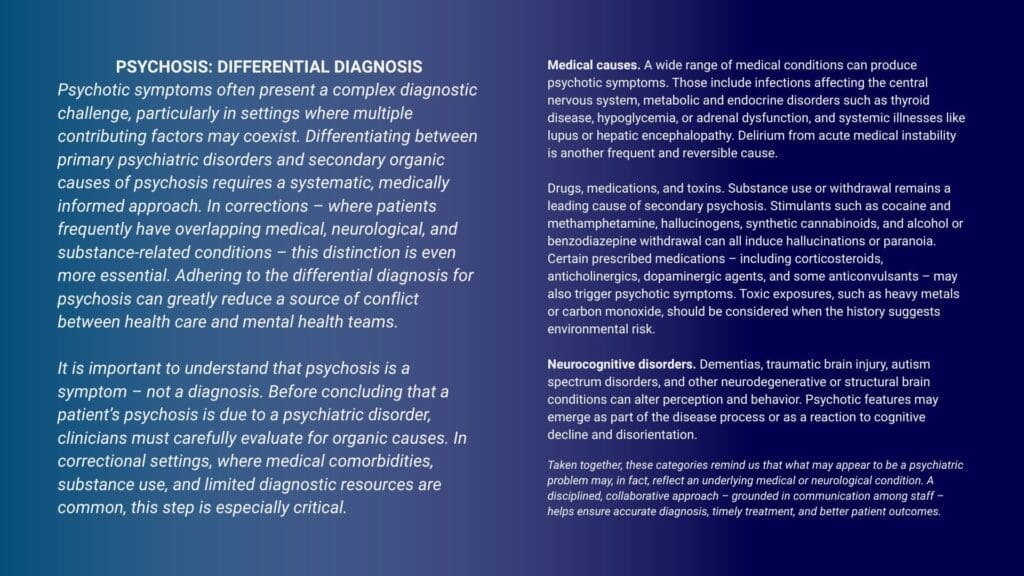
Psychotic symptoms illustrate why collaboration is essential. Before labeling psychotic symptoms as psychiatric (primary), clinicians must first rule out organic (secondary) causes such as medical conditions, substance intoxication or withdrawal, and neurocognitive disorders (see box).
For example, a patient arrived at one of our facilities appearing paranoid, disoriented, and agitated. He was initially referred for a psychiatric evaluation. Further assessment revealed tremors, diaphoresis, and elevated vital signs consistent with delirium tremens, a severe form of alcohol withdrawal. Prompt medical intervention stabilized the patient within hours.
Similar pitfalls occur in less-acute presentations. In another case, a middle-aged patient repeatedly complained of fatigue, sluggishness, and poor concentration. Medical staff, noting her flat affect and vague complaints, suspected depression and referred her to mental health. The mental health professional, however, questioned the extent of the patient’s cognitive slowing. Laboratory testing revealed significant hypothyroidism. Treatment of her hypothyroidism led to noticeable improvements in mood and energy.
Cases like those demonstrate how easily each team can rely too heavily on its own framework for understanding symptoms. When health care and mental health staff work together to review both physiological and psychological factors, they can more accurately determine whether distress is emotional, physical, or both – leading to more effective and compassionate treatment.
In correctional settings, where patients already face barriers to continuity of care and may distrust facility staff, visible disagreement among providers can further erode the therapeutic relationship. Inconsistent documentation, incomplete handoffs, and parallel treatment plans without shared decision-making diminish quality of care and increase liability risk. The most vulnerable patients – those with co-occurring disorders – are often the ones that fall through the gaps.
The effects of poor interdisciplinary communication extend far beyond clinical metrics – they directly shape how patients experience care. Incarcerated patients already live with isolation, distrust, and limited access to services. When providers disagree or cling to narrow disciplinary views, necessary interventions are delayed.
As a result, patients may feel anxious, dismissed, or unsafe. Misunderstood symptoms can lead to unnecessary restrictions or inappropriate medications, compounding stress and worsening both mental and physical health.
Conversely, when teams collaborate effectively, patients experience more consistent and compassionate care. Their trust in the entire health staff improves, and they are more likely to adhere to treatment plans and engage actively in their own recovery – advancing the larger goal of humane and effective care.
Strategies to Reduce Tension
Effective integration does not happen by accident – it takes deliberate effort from both leadership and frontline staff from all disciplines. The following strategies can help reduce tension and improve patient care.
Prioritize structured collaborations. One effective approach is to establish regularly scheduled interdisciplinary rounds, bringing together diverse health care -professionals to discuss and develop comprehensive strategies for patients with complex needs. By promoting communication and mutual understanding, interdisciplinary meetings foster integrated treatment planning. With consistent organization and leadership support, they can address time constraints and role conflicts, ultimately enhancing decision-making and building a cohesive, teambased approach to care.
Develop clear communication protocols to strengthen
how information is shared. Consistent, accurate information exchange among team members is vital. Shared electronic documentation and standardized handoff forms promote transparency and reduce miscommunication during transitions of care. Establishing clear expectations – through structured
shift reports or interdisciplinary updates – helps maintain continuity and accountability. Integrating such practices into daily workflows improves efficiency, minimizes errors, and ensures every team member has access to the same up-to-date patient information.
Invest in shared learning, including cross-training and education. Joint training on common issues – such as substance use disorders, suicide risk assessments, and somatic symptom presentations – builds mutual respect and a shared professional language. Joint sessions allow health professionals to understand each other’s roles and approaches. Fostering insight into overlapping responsibilities and complementary skills can reduce misconceptions and improve coordination. Incorporating case studies, simulations, and cross-disciplinary discussions further reinforces teamwork and consistent decision-making.
Encourage leadership commitment and modeling. Supervisors shape the culture in any professional setting. When leaders model cooperation and highlight the strengths of different disciplines, they set the tone for respect and teamwork across the facility. Their example not only reinforces shared responsibility but also encourages open communication and problem-solving. Leaders who consistently demonstrate accountability – acknowledging errors, giving constructive feedback, and supporting joint decision-making – signal that collaborative practices are valued and expected. Mentorship from leadership helps newer or less confident staff navigate interdisciplinary dynamics effectively. Recognizing and celebrating collaborative efforts builds trust, promotes a workplace culture centered on integrated, patient-focused care, and directly influences how teams handle challenging clinical situations, ultimately improving patient outcomes.
Extend collaboration to the policy level. Policies governing chronic care management, behavioral emergencies, and restraint use should be developed collaboratively, with input from both health care and mental health staff. An inclusive process helps ensure that policies are balanced, practical, and reflective of each patient’s unique needs. Shared ownership aligns ethical and clinical standards while helping to prevent gaps or conflicts in care. Regular policy reviews and interdisciplinary feedback sessions sustain consistency, compliance, and quality across all levels of care.
The Takeaway
In the demanding world of correctional health care, collaboration is not a luxury – it’s a lifeline. When handled with honesty and respect, tension between health care and mental health teams can spark development instead of division. Communication, mutual education, and shared patient-care goals can transform interprofessional friction into a foundation for more holistic and humane care.
What presents initially as a divide between teams leaves room for everyone to grow together.
Tommy Williams, BSN, RN, CCHP, is director of public relations at PrimeCare Medical.
Emily Scordellis, PsyD, CCHP, is the company’s vice president of behavioral health services.



